Introduction
Physical therapy in Brooklyn for Shoulder Issues
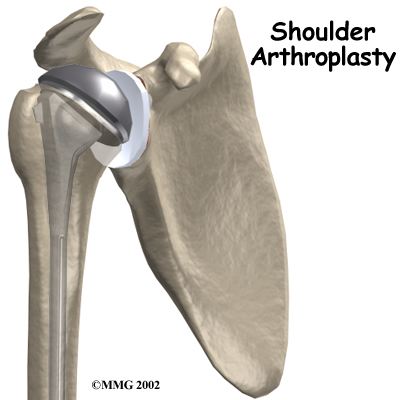
Welcome to Ari Levine PT, PC's resource on Reverse Shoulder Arthroplasty.
 Shoulder joint replacement surgery (also called shoulder arthroplasty) can effectively ease pain from shoulder arthritis. Most people experience improved shoulder function after this surgery. Unfortunately certain patients are not candidates for a traditional joint replacement of the shoulder because they lack the muscle function necessary to stabilize the joint. A different type of shoulder replacement, called a reverse shoulder replacement, may be available for many of these patients and provide pain relief as well as a stable functioning shoulder that is adequate for their daily needs.
Shoulder joint replacement surgery (also called shoulder arthroplasty) can effectively ease pain from shoulder arthritis. Most people experience improved shoulder function after this surgery. Unfortunately certain patients are not candidates for a traditional joint replacement of the shoulder because they lack the muscle function necessary to stabilize the joint. A different type of shoulder replacement, called a reverse shoulder replacement, may be available for many of these patients and provide pain relief as well as a stable functioning shoulder that is adequate for their daily needs.
This guide will help you understand:
- how the shoulder joint works
- what parts of the shoulder are replaced in a reverse shoulder replacement
- how reverse shoulder replacement differs from a regular shoulder replacement
- what to expect after reverse shoulder replacement surgery
- what Ari Levine PT, PC’s approach to rehabilitation is
Anatomy
What parts of the shoulder are involved?
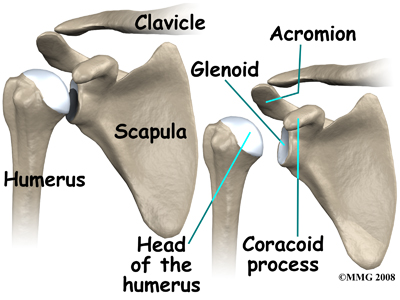 The shoulder is made up of three bones: the scapula (shoulder blade), the humerus (upper arm bone), and the clavicle (collarbone).
The shoulder is made up of three bones: the scapula (shoulder blade), the humerus (upper arm bone), and the clavicle (collarbone).
The rotator cuff connects the humerus to the scapula.
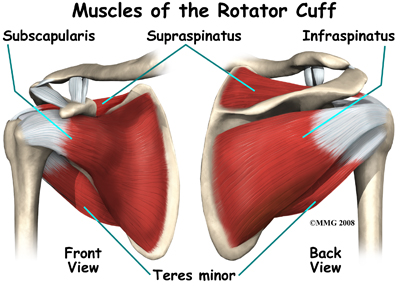
Four muscles and their associated tendons form the rotator cuff: the supraspinatus, infraspinatus, teres minor, and subscapularis.
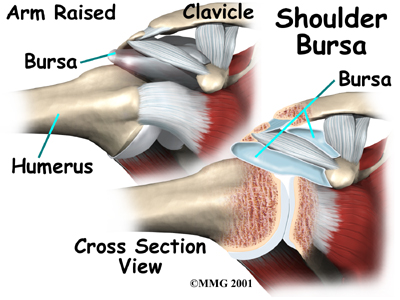
Tendons attach muscles to bones. Muscles move the bones by pulling on the tendon that they attach to. The rotator cuff muscles help raise and rotate the arm. As the arm is raised, the rotator cuff also keeps the humerus tightly in the socket. The socket of the shoulder is part of the scapula bone and is called the glenoid fossa. The glenoid fossa is very shallow and flat so without the rotator cuff muscles the top part of the humerus (the head) would slide out of the centre of the fossa.
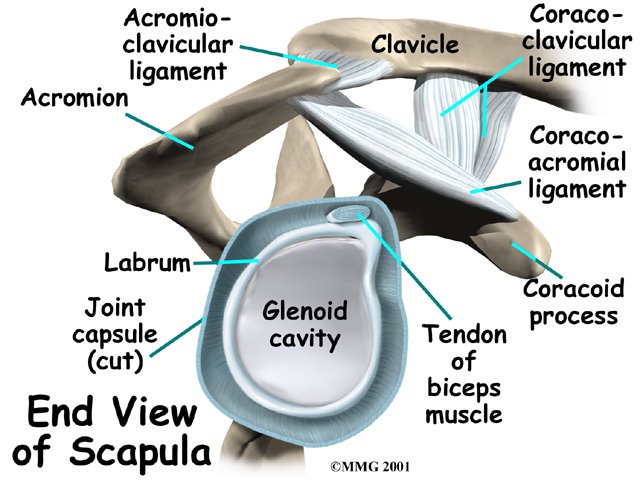
The part of the scapula that connects to the lateral shoulder is called the acromion. A bursa is located between the acromion and the rotator cuff tendons. A bursa is a lubricated sac of tissue that cuts down on the friction between two moving parts. Bursae are located all over the body where tissues must rub against each other. In this case, the bursa protects the acromion and the rotator cuff from grinding directly against each other.
The humeral head of the shoulder is the ball portion of the shoulder joint. The humeral head has several blood vessels, which enter at the base of the articular cartilage. Articular cartilage is the smooth, white material that covers the ends of bones in most joints. Articular cartilage provides a slick, rubbery surface that allows the bones to glide over each other as they move. Cartilage also functions as a shock absorber in the joint.

A watertight sac called the joint capsule surrounds the shoulder joint. The joint capsule holds fluids that lubricate the joint. The walls of the joint capsule are made up of ligaments. Ligaments are connective tissues that attach bones to bones. The joint capsule has a considerable amount of slack (loose tissue), so that the shoulder is unrestricted as it moves through its large range of motion.
Related Document: Ari Levine PT, PC's Guide to Shoulder Anatomy
Shoulder Anatomy Introduction
Rationale
What conditions lead to reverse shoulder joint replacement?
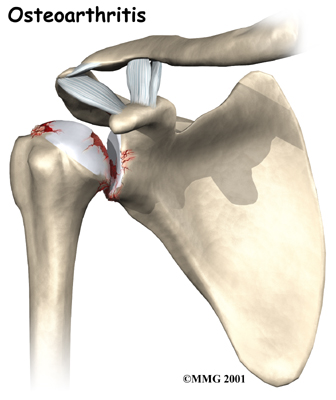
The most common reason for undergoing shoulder replacement surgery is osteoarthritis. Osteoarthritis is caused by the degeneration of the joint over time, through wear and tear. Being that the shoulder is not a weight-bearing joint, it does not suffer as much wear and tear as other joints such as the weight-bearing hip and knee joints. Although osteoarthritis in the shoulder can occur without any causative injury to the shoulder, this is uncommon; usually it is a subsequent result of another injury or disease in the shoulder joint.
Rotator cuff problems are common conditions in the shoulder, especially as we grow older. Degeneration or wear and tear of the rotator cuff tendons occurs as we age. Over time this can lead to weakening of the tendons and may result in a rotator cuff tear.
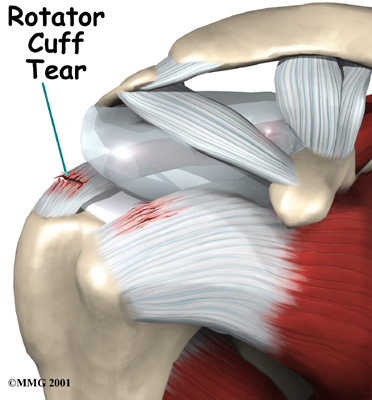 Surgery to repair a rotator cuff tear is fairly common in people who are middle aged or older. Small, medium and many large tears can be repaired either through arthroscopic or open surgical procedures. Most rotator cuff repairs are successful but in a portion of patients the torn tendon has become so degenerated that the tendon cannot be repaired. Unfortunately, many large tears that are untreated for a long time may retract which renders them unfixable.
Surgery to repair a rotator cuff tear is fairly common in people who are middle aged or older. Small, medium and many large tears can be repaired either through arthroscopic or open surgical procedures. Most rotator cuff repairs are successful but in a portion of patients the torn tendon has become so degenerated that the tendon cannot be repaired. Unfortunately, many large tears that are untreated for a long time may retract which renders them unfixable.
A shoulder joint without an intact rotator cuff may still function relatively well. Some patients will have some weakness, pain and may not be able to completely raise the arm, however, they get by without full function of their rotator cuff fairly well. There are many people who choose not to have surgery to repair a rotator cuff tear and will simply live with the limitations. Patients with massive rotator cuff tears, however, may not be able to lift the arm without significant pain and weakness, which severely limits them on a daily basis. When the arm cannot be lifted, this is called a pseudoparalytic shoulder.
A normal functioning rotator cuff helps to keep the shoulder stable so that it can move well, and also helps to create part of the joint capsule, which holds the joint fluid that lubricates the joint. Over time, a shoulder without an intact rotator cuff becomes arthritic; the shoulder joint wears out due to the abnormal motion in the joint, the instability, and the decreased joint fluid lubrication. This type of wear and tear arthritis in the shoulder is called (rotator) cuff tear arthropathy.
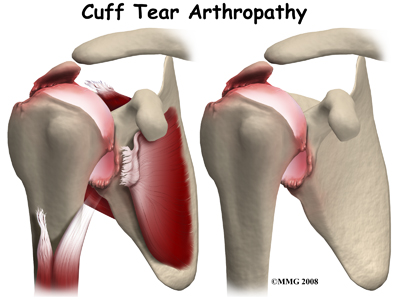 Cuff tear arthropathy is difficult to treat. The shoulder is weak and painful. Patients may not be able to raise the arm above shoulder level. Patients with this type of arthritis would seem to be good candidates for a shoulder replacement, but replacing the shoulder in the traditional fashion has not been successful.
Cuff tear arthropathy is difficult to treat. The shoulder is weak and painful. Patients may not be able to raise the arm above shoulder level. Patients with this type of arthritis would seem to be good candidates for a shoulder replacement, but replacing the shoulder in the traditional fashion has not been successful.
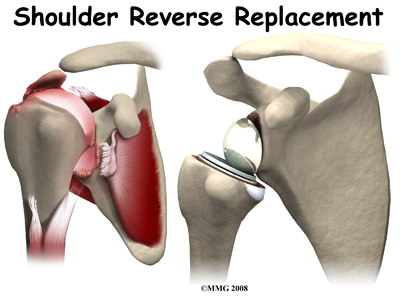
The answer to this dilemma was to rethink the mechanics of the shoulder joint and to design an artificial shoulder that worked differently than the real shoulder joint. The solution was to reverse the socket and the ball, placing the ball portion of the shoulder where the socket use to be and the socket where the ball or humeral head use to be.
This new design led to a much more stable shoulder joint that could function without a rotator cuff. The artificial joint itself provided more stability by creating a deeper socket that prevented the ball from sliding up and down as the shoulder was raised. The large deltoid muscle that covers the shoulder could be used to more effectively lift the arm, providing better function of the shoulder. The final result is a shoulder that functions better, is less painful and can last for years without loosening.
Other reasons to consider a reverse shoulder replacement include failed rotator cuff surgery leading to a pseudoparalytic shoulder even without arthritis. As mentioned previously a pseudoparalytic shoulder refers to a situation where you cannot raise the arm and shoulder. Pseudo means false and paralysis means that the nerves that control the muscle can no longer do so. A pseudoparalytic shoulder appears paralyzed, but instead of the nerve being damaged causing the paralysis, the reason that you cannot raise the shoulder is because the rotator cuff tendons (attaching to the muscles on the humerus which raise the shoulder) are torn. The power of the muscles cannot be transmitted to the humerus to raise the shoulder.
Older patients with very severe fractures of the head of the humerus are another group of patients that appear to do very well with reverse shoulder replacements as opposed to a standard shoulder replacement. Patients who have had previous shoulder replacements that have failed or become loose will also require a reverse shoulder replacement to fix the loose or painful prosthesis.
In most cases, doctors see any type of shoulder replacement as a last option for a patient. Sometimes there is a benefit to delaying shoulder replacement surgery as long as possible. Your doctor will probably want you to try nonsurgical measures to control your pain and improve your shoulder movement, including medications and physical therapy.
Like any arthritic condition, cuff tear arthropathy of the shoulder may respond to anti-inflammatory medications such as aspirin or ibuprofen. Acetaminophen or paracetamol may also be prescribed to ease the pain. Some of the newer medications such as glucosamine and chondroitin sulfate are more commonly prescribed today as they seem to be effective in helping to reduce the pain of arthritis in all joints. There are also new injectable medications that lubricate the arthritic joint. These medications have been studied mainly in the knee but are presently being studied also for the shoulder.
An injection of cortisone into the shoulder joint may give temporary relief to your shoulder. Cortisone is a powerful anti-inflammatory medication that can ease inflammation and reduce pain, possibly for several months. Most surgeons only allow two or three cortisone shots into any joint. If the shots don't provide you with lasting relief, your doctor may suggest surgery.
Physical therapy can be very useful and can assist you if you decide not to undergo surgery and live with the problem in your shoulder. If you plan to undergo a shoulder replacement, physical therapy prior to the surgery will be encouraged to help you gain as much of the motion and strength in your shoulder as possible prior to the surgery. Regular physical therapy treatment at Ari Levine PT, PC will also be required post-surgically.
Preparation
What do I need to do to get ready for surgery?
When cuff tear arthropathy of the shoulder requires replacement of the painful shoulder with an artificial shoulder joint, a reverse shoulder replacement may be recommended. You and your surgeon should make the decision to proceed with surgery together. You need to understand as much about the procedure as possible. If you have concerns or questions, you should talk to your surgeon.
Once you decide on surgery, you need to take several steps. Your surgeon may suggest a complete physical examination by your regular doctor. This exam helps ensure that you are in the best possible condition to undergo the operation.
Plain x-rays of the shoulder will allow your surgeon to evaluate the severity of arthritis and give an indication regarding the status of the rotator cuff. A CT scan or MRI is often required before any kind of shoulder replacement to determine the degree of damage to the bones (glenoid and humeral head) for surgical planning.
As mentioned above, you will need to spend time with a physical therapist at Ari Levine PT, PC who will be managing your rehabilitation after surgery. This pre-operative visit will allow your therapist to record a baseline of information. Your therapist will check and record your current pain levels, your ability to do your activities, and will measure the movement and strength of each shoulder.
A second purpose of the pre-operative visit with your physical therapist is to prepare you for your post-surgical rehabilitation. You'll begin learning some of the exercises you will use during your recovery. In addition, your therapist can help you anticipate any special needs or problems you might have at home, once you're released from the hospital.
On the day of your surgery, you will probably be admitted to the hospital early in the morning. You shouldn't eat or drink anything after midnight the night before. Come prepared to stay in the hospital for several nights. The length of time you will spend in the hospital depends a lot on how well you are doing with your rehabilitation program post-surgically.
Surgical Procedure
What happens during reverse shoulder replacement surgery?
Before we describe the procedure, let's look first at the reverse artificial shoulder itself.
The Reverse Artificial Shoulder
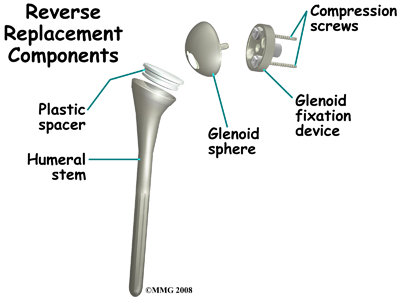 The reverse shoulder prosthesis (artificial joint) is made up of two parts. The humeral component replaces the humeral head, or the ball of the joint. The glenoid component replaces the socket of the shoulder, which is actually part of the scapula.
The reverse shoulder prosthesis (artificial joint) is made up of two parts. The humeral component replaces the humeral head, or the ball of the joint. The glenoid component replaces the socket of the shoulder, which is actually part of the scapula.
In the traditional artificial shoulder prosthesis, the glenoid prosthesis is a shallow socket made of plastic and the humeral component is a metal stem attached to a metal ball that nearly matches the anatomy of the normal shoulder. In the reverse shoulder replacement, the ball and the socket are reversed such that the ball sticks out of the shoulder itself.
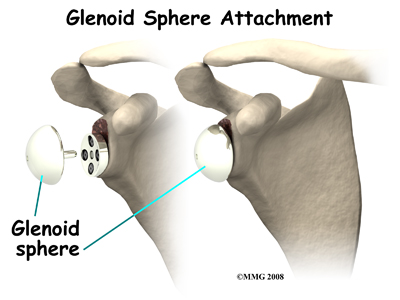
The humeral component is a combination of a metal stem that fits into the marrow cavity of the upper humerus and, on top of the metal stem, a plastic socket. This plastic socket fits onto the humeral component to create a ball and socket type bearing. The glenoid component is usually made of two parts: a metal tray and a metal ball. The metal tray (base plate) attaches directly to the bone. This base plate is inserted into a small peg hole drilled into the bone and is secured with special screws through the base plate into the bone. Attached to that metal tray, there is a metal ball that will fit into the plastic socket attached to the humeral component. The plastic is very tough and very slick, much like the articular cartilage it is replacing. This plastic is so tough that you could actually ice skate on a sheet of this plastic without causing it much damage.
The Operation
The reverse shoulder replacement surgery is performed almost identically to the traditional shoulder replacement except that different artificial parts are inserted.
You will most likely need general anesthesia for a reverse shoulder replacement surgery. General anesthesia puts you to sleep. It is difficult to numb only the shoulder and arm in a way that makes such a major surgery possible. While nerve blocks can be helpful with postoperative pain control, they are not usually effective enough to be used as the only anesthetic for this kind of operation.
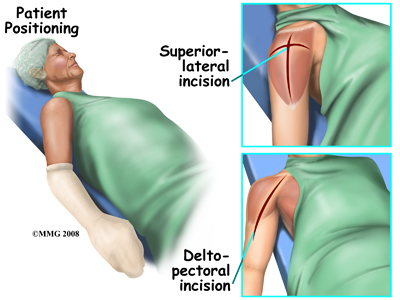 Shoulder replacement surgery is done through an incision on the front of your shoulder. This is called an anterior (deltopectoral) approach. For reverse shoulder replacements, especially for patients with multiple previous surgeries, a superior approach through the deltoid muscle may be used. No matter which approach is used, the surgeon cuts through the skin and then isolates the nerves and blood vessels and moves them to the side. The muscles are also moved to the side. If the deltoid requires cutting, a delay in your rehabilitation will be needed to allow the deltoid muscle to heal before putting stress through it.
Shoulder replacement surgery is done through an incision on the front of your shoulder. This is called an anterior (deltopectoral) approach. For reverse shoulder replacements, especially for patients with multiple previous surgeries, a superior approach through the deltoid muscle may be used. No matter which approach is used, the surgeon cuts through the skin and then isolates the nerves and blood vessels and moves them to the side. The muscles are also moved to the side. If the deltoid requires cutting, a delay in your rehabilitation will be needed to allow the deltoid muscle to heal before putting stress through it.
The surgeon enters the shoulder joint itself by cutting into the joint capsule. This allows the surgeon to see the joint. In more advanced cases of cuff tear arthropathy, and in patients with previous surgery, there may be no capsule and rotator cuff remaining.
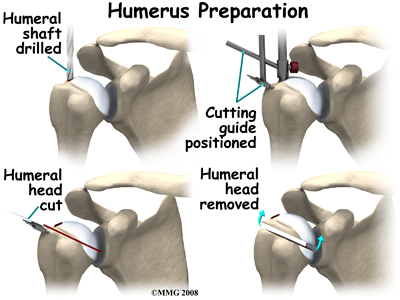
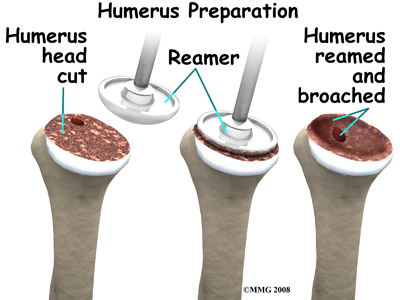
At this point, the surgeon can prepare the bone for attaching the replacement parts. The ball portion of the humeral head is removed with a bone saw. The hollow inside of the upper humerus is prepared using a rasp, which allows your surgeon to mold the space in order to anchor the metal stem of the humeral component inside the bone.
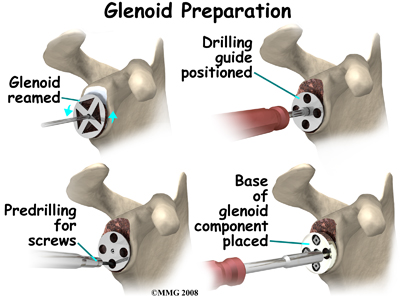
The glenoid will be replaced with a ball of metal. The arthritic glenoid surface is prepared by grinding away any remaining cartilage and flattening the surface. This is done with an instrument called a reamer. The surgeon usually uses the reamer to drill holes into the bone of the scapula and to flatten the deformed glenoid surface so the base plate rests on a smooth, flat surface. This is where the stem of the glenoid component is anchored.
Finally, the humeral component and the glenoid component are inserted.
Once the joint is anchored, the surgeon tests for proper fit. When the surgeon is satisfied with the fit, the joint capsule is stitched together. The muscles are then returned to their correct positions, and the skin is also stitched up.
Your incision will be covered with a bandage, and your arm will be placed in a sling. You will then be woken up and taken to the recovery room.
After Surgery
What happens after surgery?
After surgery, you'll be transported to the recovery room. You will have a dressing wrapped over your shoulder that will need to be changed frequently over the next few days. Your surgeon may have inserted a small drainage tube into the shoulder joint to help keep extra blood and fluid from building up inside the joint. An intravenous line (IV) will be placed in your arm to give you needed antibiotics and medication.
You arm will be placed in a sling usually with a large pillow that supports your arm in a position away from your body. Generally the sling will remain on for 3-4 weeks. In some cases, the use of the sling will be required for up to 6 weeks, particularly if a revision surgery has been completed.
Post-surgical Rehabilitation
What will my recovery be like?
Generally a physical therapist will see you the day after surgery to begin your rehabilitation program while you are in the hospital. Your therapist will make sure you are safe getting in and out of bed and moving about in your room with your sling on. Next they will prescribe specific range of motion exercises for you that you will begin immediately as long as your surgeon allows it. Your therapist will teach you how to remove your sling for your exercises and also how to put it back on after you have completed your exercises. The sling should be worn at all times except during showering and while performing rehabilitation exercises.
When the immobilizer is removed following surgery, you will experience some pain when you start to move your shoulder, wrist, elbow and forearm, and this is normal. This pain is from not using the joints very well prior to the surgery and also from the surgical process itself. The pain you feel should only be mild to moderate and any sharp or severe pain should be heeded. In addition, the muscles in your arm may already appear small and atrophied. Again, this is normal; once your strength beings to return your arm will start to look more normal again.
Simple finger, hand and wrist movements, as well as elbow and neck range of motion exercises will be prescribed to ensure you regain motion in these joints. For your shoulder, generally pendular exercises are prescribed along with passive range of motion exercises that encourage shoulder elevation (raising in front) as well as gentle external rotation. Pendular exercises assist with pain, help to maintain some shoulder range of motion, and assist in preventing unwanted scar tissue forming in the joint. These exercises are performed by leaning forward or to the side, letting the arm hang clear of the chest, and then initiating movement with your trunk so that the dangling limb passively and gently moves. This action provides some traction to the glenohumeral joint, which aids in pain relief, and also assists the shoulder into a relatively elevated motion (in relation to the trunk.) It is important that the pendular activity is done as passively as possible without initiating motion from the shoulder muscles.
The exercise should be similar to a weighted pendulum that randomly swings on the end of a piece of string. Icing your shoulder will be encouraged after your exercises as well as several other times during the day.
In cases where the reverse shoulder arthroplasty has been done as a revision to a traditionally replaced shoulder, or where the surgical approach has included cutting through the deltoid muscle, the initiation of early exercises will need to be delayed to allow a prolonged period of healing before putting the shoulder under any stress. In these cases your surgeon and therapist will direct you in regards to which exercises are initially allowed, and which should be avoided. In all reverse shoulder replacement cases the specific post-surgical protocol of your surgeon should be strictly adhered to. Each surgeon has their own protocol based on personal preference and experience, as well as surgical technique.
No matter which post-surgical protocol is followed, protecting the new joint is of particular importance after a reverse shoulder arthroplasty. Due to the biomechanics of a reverse arthroplasty there is a higher risk of shoulder dislocation following a reverse shoulder arthroplasty versus a traditional shoulder replacement. Unlike a traditional shoulder replacement, which is more likely to dislocate with the arm in abduction and external rotation, the reverse shoulder replacement is at risk of dislocation during isolated extension as well as the combined movements of extension, internal rotation, and adduction. Your therapist will review these movement precautions with you and you should refrain from putting your shoulder in any of these positions on their own or in combination for a minimum of 12 weeks post-surgically. Activities involving these positions, such as tucking in one’s shirt or performing personal hygiene of the back passage, are simple activities but can lead to dislocation so must be strictly avoided. It can be helpful in respecting these precautions by remembering that you should always be able to see the elbow on your surgical side during all activities with that arm.
Once you are managing your exercises well in the hospital, you are independent in doing most activities to care for yourself, and when your surgeon feels it is appropriate, you will be sent home. You will need to continue an extensive rehabilitation program once you are discharged from the hospital. In some cases, a physical therapist or occupational therapist may visit your home to check to see that you are safely getting around in your home and managing your everyday tasks with your arm in your sling. Your therapist may also review and assist you with your exercises at this time. If it is particularly difficult for you to get out of your home to attend physical therapy at Ari Levine PT, PC then a physical therapist may continue to visit you at your home for several treatments in order to review and advance your exercises. As soon as you are able, however, it is best for you to attend rehabilitation at Ari Levine PT, PC as there are several more modalities as well as exercise equipment that can be used in the clinic versus at home, which can expedite your recovery.
As an initial goal of rehabilitation your physical therapist at Ari Levine PT, PC will focus on relieving your pain and decreasing any swelling that may be lingering from the surgery. We may use modalities such as heat, ice, or electrical current to assist with decreasing any pain or swelling you have around the shoulder, anywhere along the arm, or into the hand. Due to some of the muscles of the neck and upper back connecting to the shoulder, you may also have pain in these regions, which we can treat in order to make movement of your entire upper body easier. We may also use massage or mobilizations for the neck, upper back, shoulder, elbow, forearm, or wrist to improve circulation and assist with any pain that may be present.
Due to the ongoing possibility of dislocation with a reverse shoulder arthroplasty, once you have begun therapy at Ari Levine PT, PC your therapist will review the shoulder motion precautions of shoulder extension, internal rotation, and adduction that will strictly need to be avoided for the first 12 weeks post-surgically, or until your surgeon advises you otherwise.
The next part of our treatment will focus on regaining the range of motion, strength, and dexterity in your wrist, hand, elbow, and shoulder. Your physical therapist at Ari Levine PT, PC will prescribe a series of stretching and strengthening exercises that you will practice in the clinic and also learn to do as part of your home exercise program. These exercises may include the use of rehabilitation equipment such as pulleys and poles for range of motion exercises, and light weights or exercise band for resistance work of your upper limb. The shoulder joint is the upper limb’s link to the rest of the body so it needs to be strong and well controlled for the limb and hand to work well. Exercises following a reverse shoulder arthroplasty will focus initially on gaining passive then active-assisted range of motion, while initiating some early light strengthening of the deltoid muscle as well as the other muscles around the shoulder blade that support the shoulder girdle. All exercises should be done with pristine technique as to not compromise the new shoulder joint. Your shoulder precautions should strictly be abided by and, in addition, once you have more range of movement you should be careful not to support your body weight at all with your surgical limb (ie: pushing off of a chair to get up or pushing a door open) nor lift much more than the weight of a coffee cup until your therapist clears you to do so.
Your physical therapist will be crucial in providing feedback during your exercises in order to ensure they are being done properly and safely. As time and range of motion progress, strengthening will become the major focus and will be advanced so that light weights or elastic bands are used and endurance of the muscles is improved. Your therapist will monitor your progress and advance your exercises as your shoulder can tolerate them. Along with more advanced strengthening exercises active range of motion of the shoulder will be encouraged in order to assist with strengthening and control of the entire shoulder girdle.
Proprioception is the ability to know where your body is without looking at it. As a result of any injury or surgery, this ability declines in function. A period of immobility adds to this decline. Although your arm and shoulder girdle are not traditionally thought of as weight-bearing parts of the body, even an activity such as assisting yourself with your arms to get out of a chair or pulling a plate from a cupboard requires weight to be put through your shoulder girdle and for your body to be proprioceptively aware of your limb.
The proprioceptive control of the scapula on the rib cage (scapulothoracic motion) is especially important in being able to use your shoulder girdle and upper limb effectively without causing further injury. For this reason, your physical therapist will teach you how to properly control your scapula during your rehabilitation exercises as well as during everyday activities. Your physical therapist will also remind you about maintaining good shoulder posture even when sitting or using your upper limb in activities below shoulder height, such as working on the computer. Rounded shoulders in this position crowds the shoulder joint and can lead to shoulder impingement and pain. Regaining proprioception of the shoulder girdle and upper limb can require concentrated work, and most people have not previously needed to focus so intently on such controlled motions of this joint. The concentrated effort of shoulder rehabilitation however, has a substantial reward; good scapulothoracic control is the key to regaining maximum shoulder girdle control and thus improved shoulder functioning while avoiding future shoulder pain.
Proprioceptive exercises might include activities such as rolling a ball on a surface with your hand, holding a weight up while moving your shoulder, or push-ups on an unstable surface. Advanced exercises may include activities such as ball throwing or catching. As often as possible, exercises will be incorporated that mimic your everyday activities such as grooming yourself and getting dressed, in addition to those activities that simulate your work or hobbies.
As rehabilitation advances most patients with a reverse shoulder replacement will be able to lift their arm with little or no pain. Some patients, however, may take many months to recover to this stage. It should be noted that with all reverse shoulder arthroplasty surgeries the return of full shoulder elevation or external rotation is not expected. A goal of approximately 105 degrees elevation should be anticipated. The amount of external rotation following surgery will be dependent on the state of the rotator cuff muscles prior to surgery. Despite the relative loss of range of motion, for most patients the ability to achieve this range of motion without pain offers a very functional shoulder, particularly in comparison to the shoulder’s pre-surgical status.
Generally rehabilitation at Ari Levine PT, PC after reverse shoulder arthroplasty goes smoothly, however, if during rehabilitation your pain continues longer than it should or therapy is not progressing as your physical therapist would expect, we will ask you to follow-up with your surgeon or doctor to confirm that the shoulder is tolerating the rehabilitation well and to ensure that there are no hardware issues that may be impeding your recovery.
Ari Levine PT, PC provides services for physical therapy in Brooklyn.
Complications
What might go wrong?
As with all major surgical procedures, complications can occur. This document doesn't provide a complete list of the possible complications, but it does highlight some of the most common problems.
Some of the most common complications following reverse artificial shoulder replacement are:
- anesthetic problems
- infection
- fracture
- dislocation
- loosening
- nerve or blood vessel injury
Anesthetic Problems
Most surgical procedures require that some type of anesthesia be done before surgery. A very small number of patients have problems with anesthesia. These problems can be reactions to the drugs used, problems related to other medical complications, and problems due to the anesthesia itself. Be sure to discuss the risks and your concerns with your anesthesiologist.
Infection
Infection following reverse joint replacement surgery can be very serious. The chances of developing an infection following artificial joint replacement are low (about one percent). Sometimes infections show up very early, before you leave the hospital. Other times infections may not show up for months, or even years, after the operation.
Infection can also spread into the artificial joint from other infected areas. Once an infection lodges in your joint, it is almost impossible for your immune system to clear it.
You may need to take antibiotics when you have dental work or surgical procedures on your bladder and colon. The antibiotics reduce the risk of spreading germs to the artificial joint.
Fracture
During the surgery, the humerus is prepared by cutting off the deformed humeral head and reaming the canal to allow for insertion of the humeral stem. The glenoid is reamed to create a bone tunnel, and flattened to seat the glenoid base plate. In patients with weak bone, fractures can occur during this part of the procedure that may require restricted activity after the surgery while the fracture heals.
Dislocation
Just like your real shoulder, an artificial shoulder can dislocate. A shoulder dislocation occurs when the ball comes out of the socket. There is a greater risk of dislocation right after surgery, before the tissues have healed around the new joint but there is always a slightly increased risk of dislocation with an artificial joint. Your physical therapist will teach you how to avoid activities and positions that tend to cause a shoulder dislocation. As mentioned above under post-surgical rehabilitation, the motions that are prone to a dislocation in a traditional shoulder replacement are different to those that will cause a dislocation in a reverse shoulder replacement therefore consultation with a physical therapist should be undertaken to ensure you are aware of the proper precautions. A shoulder that dislocates more than once may need another operation to make it more stable.
Loosening
The major reason that artificial joints eventually fail is that they loosen where the metal or cement meets the bone. A loose joint prosthesis causes pain. Once the pain becomes unbearable, another operation will probably be needed to fix the artificial joint.
There have been great advances in extending the life of artificial joints. However, most will eventually loosen and require another surgery. In the case of artificial knees, you can expect about 12 to 15 years, but artificial shoulder joints tend to loosen sooner.
Nerve or Blood Vessel Injury
All of the large nerves and blood vessels to the arm and hand travel through the armpit (axilla). Being that shoulder replacement surgery takes place so close to the axilla, it is possible that the nerves or blood vessels may be injured during surgery. The resulting problems may only be temporary if the injury was caused by stretching of the nerves to hold them out of the way during the surgery. The nerves and blood vessels rarely suffer any kind of permanent injury after reverse shoulder replacement surgery, but this type of injury can happen.
Portions of this document copyright MMG, LLC










